The pupil is chronically large at all times and is effected by the sympathetic nervous system.
Dilation of pupils – mydriasis – when in daylight or artificial illumination, their diameter is more than 4 mm (that is more than 33 % of the iris diameter), and can be caused by several reasons:
* Paralysis of the pupils sphincter in the injury of parasympathetic pupil innervation (no reaction on light, piloracpine does not have the influence on the diameter of pupil);
* Irritation of sympathetic pupil innervation (spastic option of mydriasis – in so doing the reaction on light still be present);
* Dysfunction of pupils sphincter in case of not working afferent pupillary neurons, and, to the lower extent, mesencephalic internuncial neurons (pilocrpine stimulates constriction of pupils).
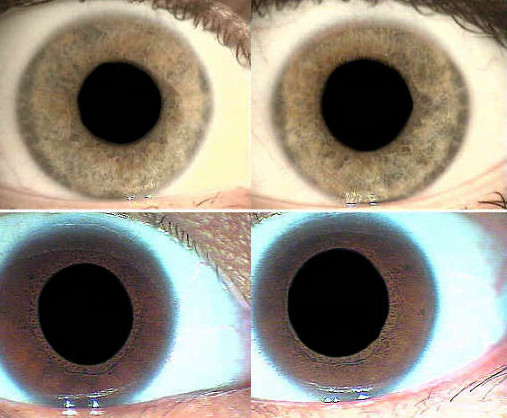
Mydriasis, or dilation of the pupils, occurs normally in daylight or artificial illumination. When the pupil diameter is more than 4 mm (more than 33% of the iris diameter), mydriasis can occur for several reasons:
* Paralysis of the pupil sphincter in the injury of parasympathetic pupil innervation (no reaction to light, pilocarpine does not have influence on the diameter of pupil)
* Irritation of sympathetic pupil innervation (spastic option of mydriasis, a state in which the reaction to light can still be present)
* Dysfunction of pupil sphincter in the case of non-working afferent pupillary neurons, and, to a lower extent, mesencephalic internuncial neurons (pilocarpine stimulates constriction of pupils)
The reasons for physiological mydriasis, besides those similar to physiological miosis (constitution, age, refraction), can be as follows:
* Sexual (differences no bigger than 0.25 mm, take place only in people with light eyes)
* Pain (associated with the increased secretion of adrenaline)
* Emotional (pleasure, fear, irritation, anger, indignation, increased attention, desire etc.)
* Vestibular-pupillary (irritation of vestibular apparatus causes long dilation of pupils after small transient constrictions)
* Cochleo-pupillary
* Promortal (moment of death and first two to three hours after it)
Pathological mydriasis appears because of different etiologic and pathogenetic factors:
* Comatose states (thyrotoxic, epileptic, eclamptic, liver, hypochlorinemic)
* Endocrinopathy (Basedow’s disease)
* Severe infectious diseases (botulism)
* Lingering pain syndrome
* Irritation of meningeal membrane (Flatau symptom)
* Visceral diseases, accompanied by hyperthermia, hypertensive crisis, dyspnea
* Intoxications (alcohol, narcotic hallucinogen, carbon disulfide, dinitrophenol, etc.)
* Pharmacological action (adrenomimetic drugs, anticholinergic novocain etc.),
* Hysterical fit (Raedlich’s symptom)
* Associated conditions including adrenal exhaustion, urinary tract disorders, bronchial disorders, and faulty digestive systems.
Unilateral mydriasis is of interest for topic diagnosis of the central nervous disease system and is a part of a number of syndromes: Pty’s, Notnaghel’s, superior orbital fissure, external wall of sinus cavernous, Webber’s, Benedict’s, neuritis of optic nerve and paralysis of oculomotor nerve, as well as post-traumatic encephalopathy.
Diagnosis of unilateral miosis or mydriasis, which is a part of multi-component clinical syndromes, is rather easy. Difficulties take place in differential diagnoses of mono-symptom and isolated unilateral miosis or mydriasis. In such cases, pharmacological tests are applied (adrenaline or homatropine).